
Omicron and subvariants have become the dominant form of Covid-19 circulating in most parts of the world. So-called bivalent mRNA vaccines became available from both Pfizer and Moderna in August or September 2022. Intended for booster vaccination, they contain mRNA both for the spike protein of the original Wuhan strain and for that of the Omicron variants BA.4 and BA.5. It was hoped these would provide additional immunity against Omicron variants, as the early trials promised.
The Swiss government made the bivalent booster available free of charge to everyone aged 16 and over and I was boosted (for the third time) with it on 5 December, just over 5 months after my previous booster. A study published by CDC in November 2022 found that the bivalent booster provided significant additional protection against symptomatic covid infection in people who had had from 2 to 4 previous monovalent vaccinations. Another study published in NEJM found that the booster was effective at reducing hospitalization from severe omicron infection by 60% (NEJM)
So I was surprised to come across another perspective published in NEJM which quoted research finding no significant difference in the immune response elicited by monovalent and bivalent vaccines and arguing that the bivalent booster should be reserved for older adults and high risk groups. I took a closer look at the benefits of the bivalent booster using data from the CDC COVID Tracker on rates of COVID-19 cases and deaths by vaccinations status.
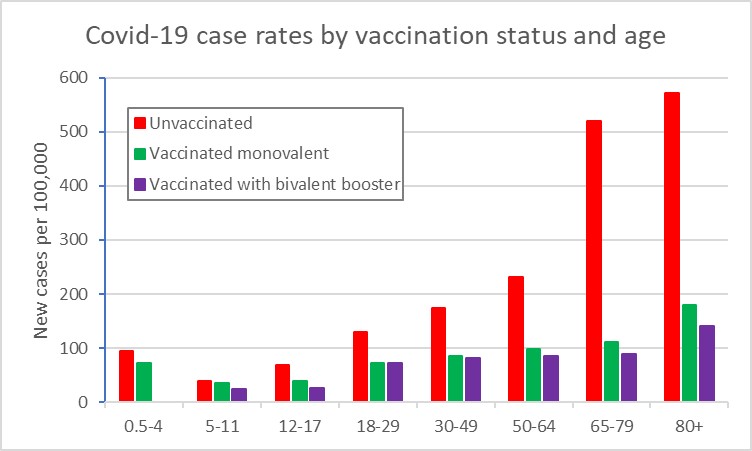
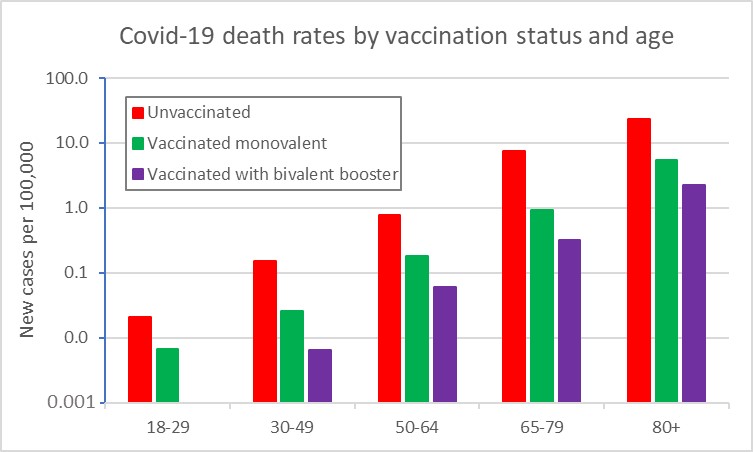
I aggregated data on cases detected in the nearly 3-month period from 1 October to end of third week of December 2022, and calculated average case and death rates by vaccination status and age group. The first figure shows case rates and the second death rates by vaccination status. Note that the death rates are plotted on a logarithmic scale. The bivalent booster provides additional protection against infection mainly for the older age groups from 50 onwards. It provides a substantial additional protection against death across all age groups from 30 onwards, although death rates are much lower for 30-49 than for 50 and over.
The following table compares the relative risk of infection and death for the unvaccinated and the monovalent vaccinated compared to the bivalent boosted as the standard:
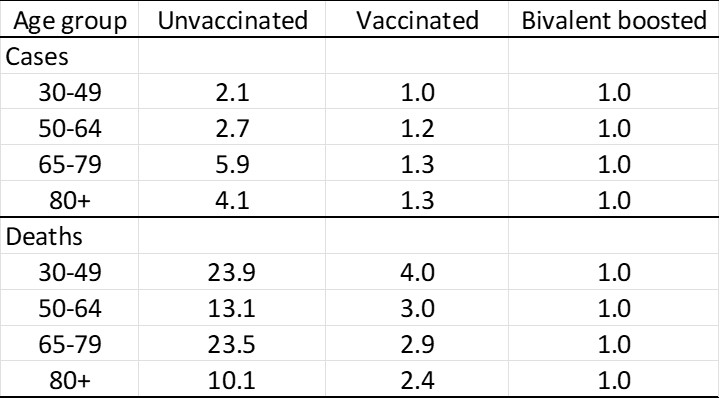
For my age group, the bivalent booster reduces the risk of infection to 1/6th and the risk of death to nearly 1/24th that of the unvaccinated. It reduces my risk of infection by 25% compared to the monovalent vaccinated, and the risk of death to one-third that of the monovalent vaccinated. Seems worthwhile additional protection to me.
