
In my previous post, I estimated that 47% of pregnancies are unintended, and of these, 43% occur in countries where abortion is illegal or severely restricted. Globally, 60% of unintended pregnancies are aborted. In countries where abortion is widely available, 71% of unintended pregnancies are aborted compared to 46% in countries with severe restrictions.
The World Health Organization (WHO) estimates that around one-third of the 23 million induced abortions carried out each year in countries where abortion is severely restricted are performed under the least safe conditions, by untrained persons using dangerous and invasive methods. Safe abortion is an essential health care service. It is a simple intervention that can be effectively managed by a wide range of health workers using medication or a surgical procedure. In the first 12 weeks of pregnancy, a medical abortion can also be safely self-managed by the pregnant person at home.
I’ve been involved in the estimation of global deaths due to maternal mortality for WHO and UNICEF since the early 2000s. WHO defines maternal mortality as death while pregnant or within 42 days of the end of pregnancy from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes. This measure is reported by WHO and UNICEF as a maternal mortality ratio per 100,000 births (MMR) for international comparisons and monitoring.
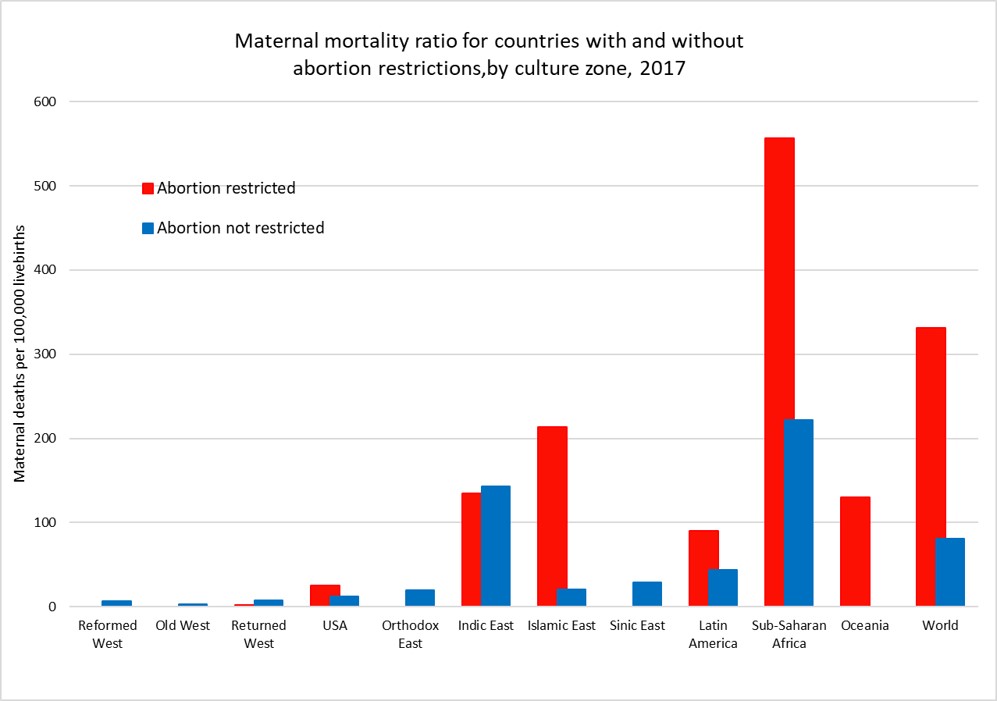
The following plot shows average MMR for countries grouped by access to abortion and country zone for the year 2017. US states have been grouped according to abortion restrictions and state-level MMR estimates from GBD2019 used and adjusted to match the national average MMR reported by CDC. Only one country, Poland, in the three “West” culture zones restricts abortion and it has an apparently very low MMR. While countries that restrict abortion have higher MMRs than those that don’t for most of the culture zones, we cannot conclude that abortion restriction per se is responsible for the difference. Abortion restriction is also correlated with other determinants of higher MMR such as lower average income per capita, less access to health care, and higher levels of discrimination against women.
The global MMR has declined from 345 per 100,000 livebirths in 2000 to 212 per 100,000 livebirths in 2017, a 40% decrease in 17 years. There have been substantial declines in MMR in every culture zone except for the Reformed West and Old West where MMR rates were already very low in 2000 and in the USA where rates have risen substantially during the 21st century. The plot below takes a closer look at MMR trends in the USA, the Reformed and Old West, the Returned West and the Orthodox East. The latter two culture zones include the former Soviet bloc countries. With the exception of Poland in the Returned West, all these culture zones except the USA do not restrict access to abortion services and allow abortion on request or in some countries on “economic and social grounds”.

WHO/UNICEF estimates of MMR have been extended forward to 2019 using trend estimates from GBD2019. The US MMR estimates have been adjusted for consistency with CDC statistics on MMR for years 2000 to 2020. The maternal mortality ratio for the USA has increased from around 15 per 100,000 livebirths in 2000 to 23.8 in 2020, a 62% increase. Abortion rates in States which now restrict abortion were similar to those in states which don’t until 2008 and afterwards diverged substantially. The rate for states with restrictions was 26.4 in 2020, 30% higher than the MMR of 20.2 for states without restrictions.
There has been considerable controversy about the substantial increase in maternal mortality in the USA, particularly as to whether it is associated with improvements in the identification and reporting of maternal deaths. Identification of pregnancy-related deaths has improved over time due to the use of computerized data linkages between birth and death records, and the addition of a pregnancy checkbox to death records from 2003 onwards. This checkbox is thought to have led to some increase in estimated MMRs in the early 2000s, but several studies have also identified that increasing restrictions on the general availability of reproductive health services have played a major role in the substantial increase in maternal mortality seen in the USA, particularly in states restricting access to abortion.
Hawkins et al (2019) found that a 20% reduction in the numbers of Planned Parenthood clinics resulted in an 8% increase in maternal mortality and states that enacted legislation to restrict abortions based on gestational age increased the maternal mortality rate by 38%.
A 2020 study by the Commonwealth Fund compared maternity care in the USA with 10 other developed countries and found that the USA has the highest maternal mortality among developed countries and that there is an overall shortage of maternity care providers (obstetrician-gynecologists and midwives). The USA has 12 to 15 providers per 1,000 livebirths, and all the other developed countries have a supply that is between two and six times greater. Although a large share of its maternal deaths occur postbirth, the U.S. is the only country not to guarantee access to provider home visits or paid parental leave in the postpartum period.
In the first five or so years I was at WHO, I worked with a maternal health colleague who provided estimates of deaths due to unsafe abortions using very uncertain estimates of the numbers of unsafe abortions and literature reviews of studies of death rates associated with unsafe abortion. Unsafe abortion was estimated to account for around 13% of total global maternal deaths, which were then estimated to be around half a million deaths per year at the beginning of the 21st century.
A more recent study by WHO staff and academic colleagues in 2014 estimated that abortion accounted for 7.9% of maternal deaths at global level between 2003 and 2009 (with uncertainty range 4.7 to 13.2%). An estimated 287 000 maternal deaths occurred worldwide in 2010, most of which were in low-income and middle-income countries and were avoidable. This would suggest there were around 22,700 maternal deaths per year associated with abortion.
Recent WHO estimates for global deaths by cause do not include deaths due to induced abortion. The IHME Global Burden of Disease Study 2019 has produced estimates of maternal deaths due to abortion and miscarriage for the period 1980 to 2019. These would also include induced abortion deaths as well as deaths due to spontaneous abortions and miscarriages.
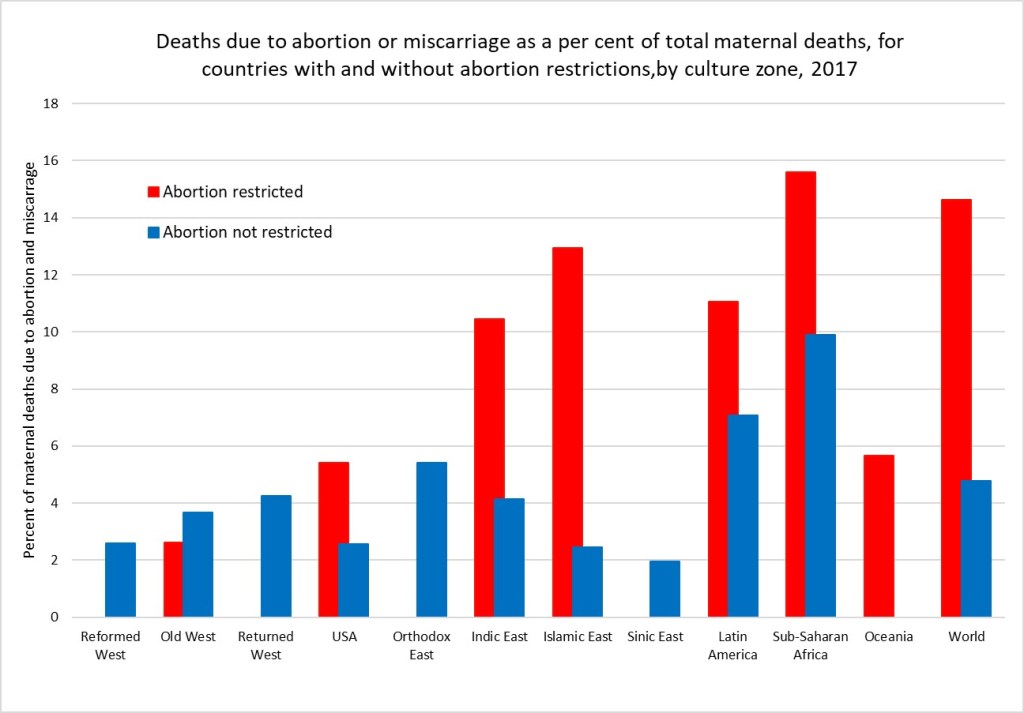
I have used IHME GBD estimates of the proportion of maternal deaths that are due to abortion and miscarriage to impute estimates for these deaths consistent with the latest available WHO/UNICEF estimates of maternal deaths for all countries for the year 2017. The figure below shows the average percent of maternal deaths attributed to abortion and miscarriage for countries with and without abortion restrictions in each culture zone.
Overall, I estimate that there were 75,500 deaths globally due to abortion and miscarriage in 2017 (these include spontaneous events as well as induced abortions). Of these 70,300 were in countries with abortion restrictions. I’ve done a very back of the envelope approximation of the abortion deaths that might be attributable to unsafe abortion by making the big assumption that the percent of deaths due to spontaneous abortion and miscarriage are the same as those for the countries in the region for which abortion access is not restricted. The excess deaths are then attributed to unsafe abortion. I estimate that abortion restrictions resulting in unsafe abortions caused 54,350 deaths in 2017. If all abortions were safe, there would have been only 21,200 deaths due to spontaneous abortion and miscarriage in 2017.
At global level, 4.8 per cent of maternal deaths are classified as due to abortion or miscarriage (spontaneous or induced) In countries without abortion restrictions and 14.6% in countries with restrictions. Adjusting to removed estimated spontaneous events, I estimate that 6.9% of maternal deaths in countries with abortion restrictions are due to unsafe abortion. Its quite possible these very back-of-the-envelope estimates are under-estimates. Classification of maternal deaths due to abortion, and more specifically unsafe abortion, is associated with a risk of misclassification. Even where induced abortion is legal, religious and cultural perceptions in many countries mean that women do not disclose abortion attempts and relatives or health-care professionals do not report deaths as such. Under-registration of deaths might be the result of stigmatisation of abortion affecting what information is reported by relatives and informants or intentional misclassification by providers when abortion is restricted. In these circumstances, the overall number of maternal mortality might not be affected, whereas abortion-related deaths might be significantly underestimated because of this under-reporting.
