Sam Preston and Yana Vierboom published a short paper in April which showed that Americans die at higher rates than Europeans and this translated into roughly 400,000 additional deaths in 2017 that would not have occurred if the USA had Europe’s lower age-specific death rates. That is about 12% of all American deaths and higher than the COVID-19 death toll of around 380,000 in 2020. In a recent Guardian article, they summarized this as “The mortality penalty that the US pays every year is equivalent to the number of Americans who died of Covid in 2020”. They also note that because people tend to die at older ages than those characterizing excess deaths, the total potential years of life lost are three times greater for the excess deaths than for Covid in 2020 (13 million versus 4.4 million).
In the Guardian article, they identify a number of factors that contribute to these excess deaths: overweight and obesity, the deaths of despair identified by Case and Deaton (drug overdose, suicide and alcohol-related causes) and lack of universal health insurance (see here and here). These factors have been widely identified as contributing to higher mortality rates and lower life expectancy for the USA compared to high income European countries, but their comparison of this mortality gap with the Covid death toll was a compelling way to present it. So I was interested to replicate and update their analysis and try to make ballpark estimates of the contribution of these factors to the excess deaths.
Preston and Vierboom used data from the Human Mortality Database (HMD) to create a composite of the five largest European countries, whose combined population size is very similar to that of the United States: Germany, England and Wales, France, Italy, and Spain. Additionally, they argued that using these larger European countries to provide a mortality standard would avoid unrealistic expectations for a larger and more diverse population that might result from comparisons including small countries where there may be exceptional combinations of factors affecting mortality (e.g., climate, diet, social history, and healthcare delivery) Their analysis covered the period 2000 to 2017, the latest year for which data were available for all six countries.
I downloaded data for these countries from the HMD a few days ago, and mortality rates were available for all six up to 2017, for four for 2018, and only the USA for 2019. I projected (non-Covid) age-sex specific mortality rates forward to 2020 and added Covid deaths for 2020 using age-sex distributions published by European countries by INED. I then adjusted the projections and in some cases the added 2020 Covid deaths to match the sex specific life expectancies at birth and at age 65, published by Eurostat up to and including year 2020. Data for non-Covid and Covid mortality by age and sex in 2020 were taken from national statistical office sources for the UK and USA.
Figure 1 below shows the ratio of US death rates to the average death rates* for the five European countries (the “European standard”) by age, in 2000, 2010, 2019 and 2020. US mortality rates are consistently higher than the European standard for all ages below 80 years and the ratio has gotten progressively worse throughout the 21st century. The ratio peaks among 25-29 year olds at almost 3 in 2019 and 3.24 in 2020.
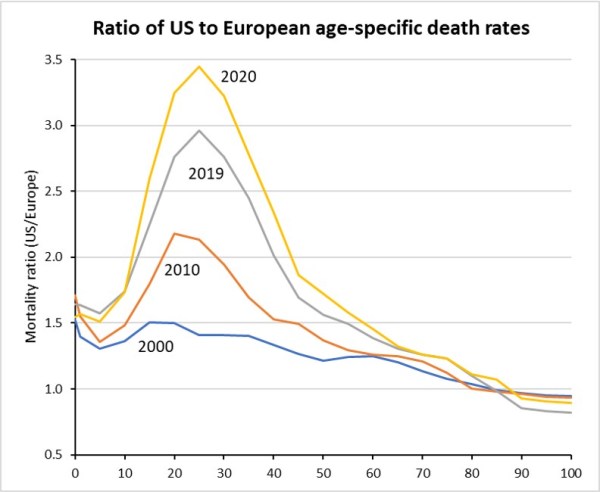
Figure 2 below shows the annual trend in total excess deaths in the USA above the number than would have occured if the US population had been subject to the age-sex specific death rates of the European standard. This excess rose from 219,000 in the year 2000 to 410,000 in 2019 and 616,000 in 2020. Although there were over 380,000 Covid deaths in the USA in 2020, the European standard also includes substantial numbers of Covid deaths, and the Covid excess for the USA is “only” 136,000 deaths.
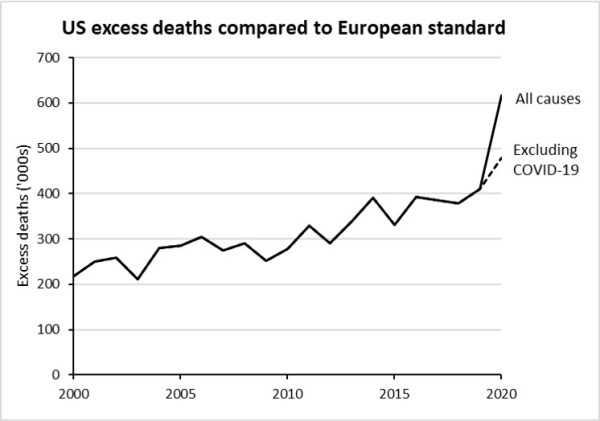
Figure 3 shows the age pattern of US excess deaths in 2000, 2010 and 2020. Although the death rate ratio is highest in the 25-34 year age group, overall death rates rise with age and the peak in excess deaths is at older ages from around 40 to 75 year. From age 90 onwards, US death rates are somewhat lower than the European standard. Thus the excess deaths below age 90 are actually higher than the total excess and in 2020 there were 764,000 excess deaths below 90, of which 99,000 were Covid-90 deaths.

In their Guardian article, Preston and Vierboom identified several factors that contribute substantially the US excess. I have made approximate estimates of the contributions of these factors using estimates from the Global Burden of Disease 2019 update (IHME GBD2019) of death rates by age and sex for the six countries for drug overdose, suicide, homicide, deaths attributable to overweight and obesity, deaths attributable to alcohol and drug use.
The 2019 age-sex specific percentages of deaths attributable to these causes were also applied to the 2020 non-Covid mortality estimates. Numbers for drug use were adjusted to reflect a 13% increase in drug overdose deaths in 2020 compared to 2019, an approximately 25% increase in homicide deaths and a 5% decrease in suicide deaths.
Unlike the USA, all the European countries have universal healthcare insurance. The number of working age Americans without health insurance rose from 38.7 million under age 65 in 2000 to 46.5 million in 2010 and then dropped to around 26 million following the introduction of Obamacare. Around 1% of Americans aged 65 or more are also uninsured. The number uninsured has risen to around 30 million in 2020 due to Republican efforts to restrict and dismantle Obamacare. I used an estimate of the hazard ratio for mortality among the uninsured compared with the insured, of 1.4 to calculate the excess mortality among the uninsured. This figure includes adjustments for age, sex, body mass index, alcohol use, smoking, and a number of other factors. The ratio was 1.8 adjusted for age and sex only.
In addition to the uninsured, a substantial number of Americans are underinsured, defined as having out-of-pocket and deductible expenses greater than 10% of their income. Apart from substantial problems with debt, around half of the underinsured do not get needed care because of cost and there are associated excess deaths (see here and here). The number of Americans underinsured has risen from around 16 million prior to Obamacare to around 30 million in 2020. I assume a mortality ratio of 1.1 among the underinsured.
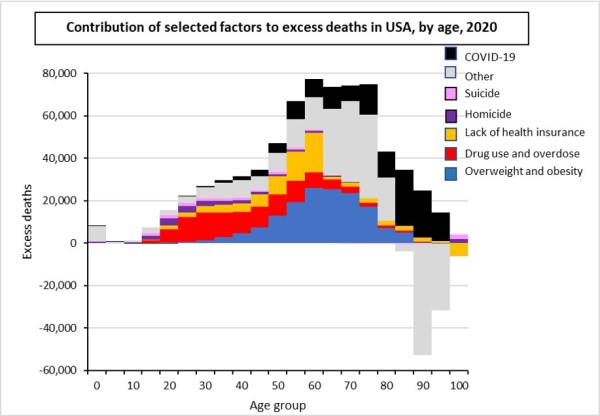
Figure 4 shows the approximate contributions of overweight and obesity, drug use and overdose, suicide, homicide, lack of health insurance and Covid to the US excess deaths relative to the European standard. Together these six factors account for around 80% of the excess deaths. Excess deaths due to alcohol use were not included as a separate factor in this graph because European and US death rates were quite similar, and the alcohol excess was small and actually negative in 2000.
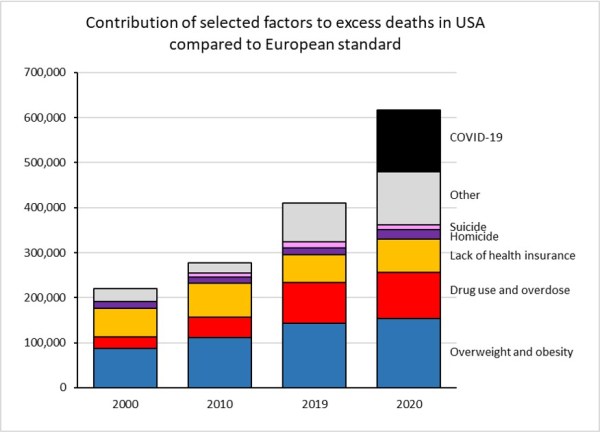
For 2020, the leading cause of excess deaths was overweight and obesity (around 154,000 deaths), followed by Covid-19 (136,000 deaths), drug use and overdose (103,000 deaths) and lack of health insurance (74,000 deaths). Excess deaths due to homicide and suicide were smaller at 20,200 and 11,200 respectively. If the USA had the European standard death rates for gun homicides and gun suicides, it would have 15,900 fewer gun homicides and 19,200 fewer gun suicides. Around 42% of the latter would still commit suicide by other means.
Figure 4 also illustrates the dramatic rise in drug overdose deaths, the vast majority due to opioids both prescription and illicit, which has occurred over the last decade. In a previous post, I examined this in more detail and noted that, in 2019, the USA accounted for an astonishing 40% of estimated global drug deaths.
Figure 5 shows the age distribution of each of the six factors contribution to total excess deaths in 2020. Not surprisingly, excess deaths due to drug use fall predominantly among younger adults, whereas deaths due to overweight and obesity fall more in later middle and older ages.
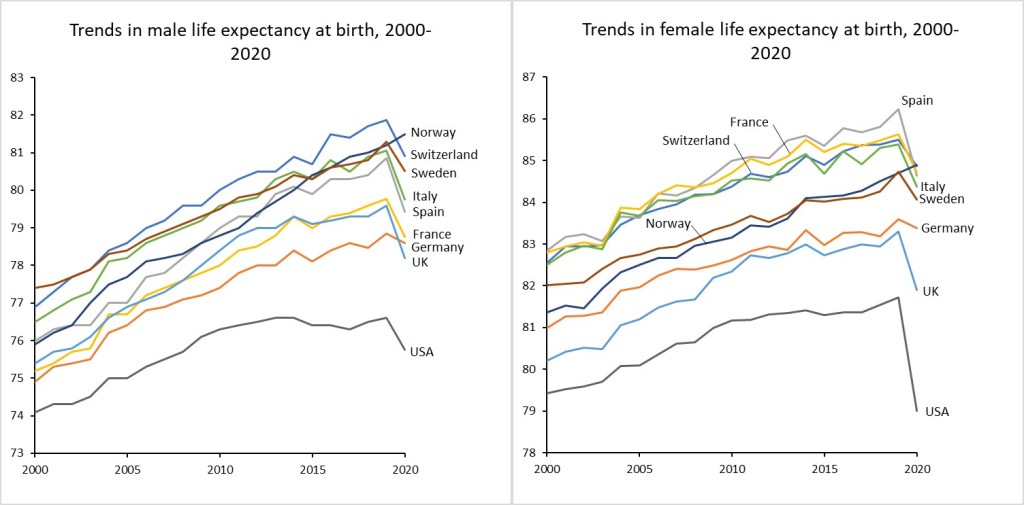
Excluding excess Covid deaths, there were almost half a million excess deaths in the USA in 2020 compared to the US standard. While overweight and obesity is not an easy problem to address, the European experience shows that substantial reductions in excess death can be achieved through introduction of universal health insurance, effective public health and other policies relating to drug use, and effective gun control. Overall, the excess deaths resulted in a life expectancy reduction for Americans of 4.3 years for males and 5.8 years for females, in 2019 before Covid caused extra reductions – see the final figure below.
Note: Most of the estimates for 2019 and 2020 in this post are based on provisional figures and have varying degrees of uncertainty. I plan to refine and improve some of the inputs and calculations, and final results may change a little. The big picture is unlikely to change significantly. In particular, the estimated total Covid deaths for 2020 may change as improved analyses are carried out on complete death registration data. The US had a significant rise in death rates for causes other than Covid-19 in 2020 and some of this may turn out to be undiagnosed Covid deaths. This will not make major differences to the provisional decomposition shown above.
